Here is a sample that showcases why we are one of the world’s leading academic writing firms. This assignment was created by one of our UK literature review writers and demonstrated the highest academic quality. Place your order today to achieve academic greatness.
Table of Contents
The objective of this dissertation is to evaluate the discriminant indices for identifying the difference between iron deficiency anemia and thalassemia minor. This research topic is based on a medical study. It analyses the causes of iron deficiency anemia. The impact of iron deficiency anemia is also expressed, and the symptoms of IDA are stated.
On the other hand, the causes and symptoms of thalassemia minor are pointed out, and even preventive measures for thalassemia minor are stated. This research paper also shows the negative impacts of IDA and thalassemia minor to analyze the discriminant indices to distinguish IDA from thalassemia minor.
The literature review defines the distinction between IDA and thalassemia minor, which will help the readers to find out the impacts and the preventions to cure. The discussion will be done by forming a critical review where opinions are taken from different scholarly sources. In order to evaluate the gravity of the topic, the researcher derives scholarly views so that the standard of the research paper should be acknowledged.
Moreover, a hypothetical statement is given for future assumptions. The research questions are stated to provide a clear view of the research objective of analysing the discriminant indices through identifying the difference between IDA and thalassemia minor. The evaluation helps the researcher to find some aspects for future reference.
This research paper’s objective is to evaluate the discriminant indices by identifying the difference between iron deficiency anemia and thalassemia minor.
This research paper is formulated depending upon some questions. The research questions can be stated as,
1. How can the discriminant indices help distinguish Anemia and thalassemia minor?
2. What are the reason behind iron deficiency anemia and thalassemia minor?
3. How issues of Anemia and thalassemia minor can be cured?
Microcytic Anemia is caused due to lack of oxygen in body cells. This type of Anemia is seen as the cells lack hemoglobin when enough red blood cells are incapable of developing in body cells. Microcytic Anemia generates both iron deficiency anemia and thalassemia minor, as in both cases, a disorder in hemoglobin is located (Gotter, 2021).
Microcytic Anemia is caused mainly due to the iron deficiency anemia (IDA) of the trait of thalassemia or an amalgamation of these. IDA is most commonly found in developing countries due to low nutritional status and in western or developed countries (Jahangiri et al. 2019).
Anemia has become a global problem. Iron deficiency anemia can be seen in a decreased hemoglobin level (Hematology, 2021). Red blood cells of the human body carry oxygen to the tissues with the help of hemoglobin. The lack of iron in body cells prevents the red blood cell from carrying enough oxygen to different parts of the body; hence the amount of hemoglobin decreases, and it gradually destroys red blood cells.
It is a slowly developing problem in the human body as it takes time to be used the stored iron of the body. The bone marrow produces fewer red blood cells with decreasing iron (Braunstein, 2020). When all the stored-up iron is used, the human body produces fewer red blood cells; hence, the body lacks oxygen supply. The symptoms of iron deficiency anemia are fatigue, weakness, shortness of breath, pale skin, drowsiness, cravings to eat dirt, clay, or ice, tingling feeling in leg, headaches, cold hands and feet, soreness, brittle nails, and irregular heartbeat.
Blood loss is one of the leading causes of IDA. The women in the premenopausal state, pregnant women, suffer from iron deficiency anemia as menstrual bleeding is the cause of iron loss (Braunstein, 2020). People who follow a low diet can also face iron deficiency as food is an iron supplier to the human body (DeLoughery, 2017). The people who donate blood, premature born babies, and vegetarians who do not eat supplements for meat are the victims of iron deficiency anemia.
The symptoms of iron deficiency anemia can be categorized as weakness or exhaustion, excess fatigue, paleness in the skin, fast heartbeat and chest pain, headache, drowsiness, and shortness of breath. Also, cold hands and feet, sore throat, craving to eat non-nutritive things such as dirt, clay, and ice, brittle nails, and poor appetite in the case of infant and child.
Insufficient iron in the diet, food provides iron to the human body. Taking iron through food is necessary. Most of the time, vegetarians do not supplement the iron of meat through any other food. This causes a deficiency of iron. Improper diet cannot ensure iron to the body that also causes iron deficiency anemia.
Menstruation and pregnancy after pregnancy, the menstrual cycle proceeds for an extended period. The woman losses blood, and that causes deficiency. Not only that, the menstrual cycle of every adult can cause iron loss. This can be the cause of iron deficiency anemia. Inability to take iron, several diseases and surgeries create problems in absorbing iron through the intestine. This can also cause a deficiency of iron in the human body.
Internal bleeding has been considered as one of the significant reasons for iron deficiency anemia. Medical issues such as colon cancer, ulcer in the stomach, and polyps in the intestine can cause internal bleeding, leading to iron deficiency anemia. Immature childbirth in the case of immature birth, the infant suffers from a deficiency of iron as the supply of iron from the mother’s cells is not complete. The child suffers from iron deficiency anemia.
Especially where the childbearing age of women is mainly diagnosed with IDA (Arora et al. 2016). This occurs because of the intermittent blood damage in the amalgamation along with deficiency of iron consumption. Thalassemia has its prevalence more in the Mediterranean regions, especially the Middle-East, Southeast Asia, Arabic peninsula countries.
Nowadays, the population relocation also has spread to a large extent that has distributed the thalassemia spread nearly in all parts of the universe (Carla et al. 2020). Thalassemia can be defined as an inherited disorder in the blood (Holm, 2020). This creates hemoglobin disorder in the blood, which destroys RBC or red blood cells (Holm, 2020).
The oxygen supply level of RBC decreases because of this reason, and the person suffers from thalassemia. Thalassemia is inherited, which means the parents or only one parent carry thalassemia to their child. The patients who have minor thalassemia bear a part of the beta-thalassemia gene. This kind of thalassemia can be described as a part of Anemia.
The mild iron deficiency can be the cause of thalassemia minor. The persons with thalassemia minor are found to have an average iron level. Thalassemia minor can be familiarised with Anemia, but there are differences, such as thalassemia is inherited and IDA is acquired. The case of thalassemia minor is not taken to be much serious in medical science as it can be controlled with some medicines and proper diet. Still, severe issues occur due to blood loss in the case of Anaemia.
Professional editors proofread and edit your paper by focusing on:
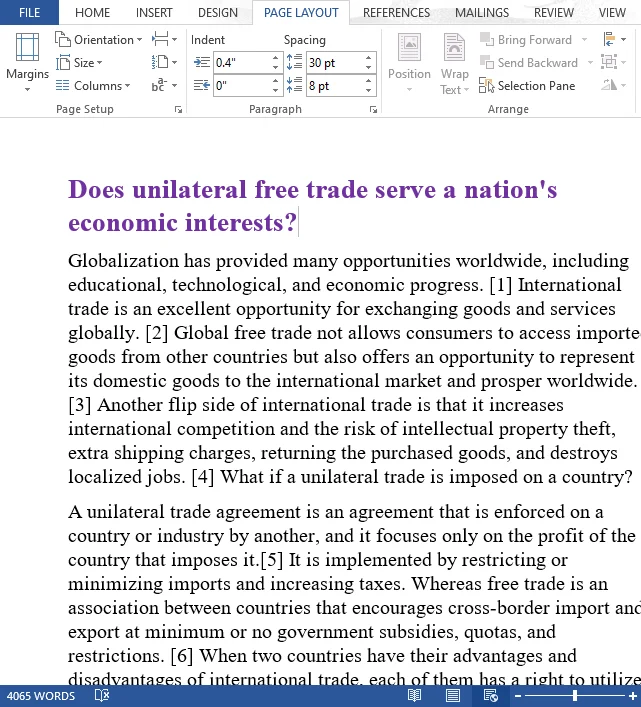
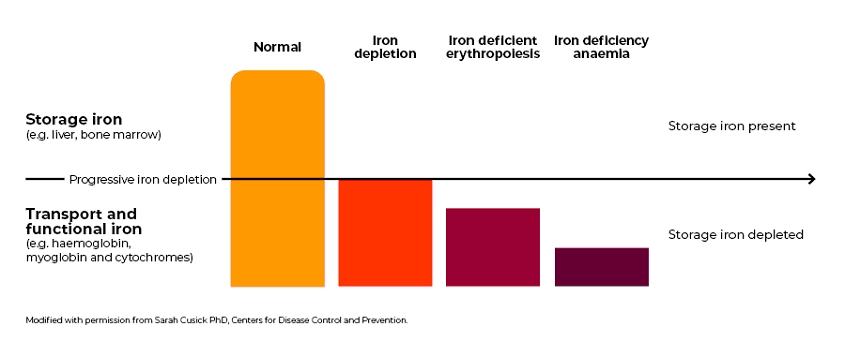
Figure 1: Iron deficiency stages
Source : (Transfusion, 2020)
The symptoms of Thalassemia Minor such as Pale skin, shortness of breath, dizziness, and fatigue. Cramps in the leg, chest pain, headache, poor feeding, fast heartbeat, delayed growth, cold hands and feet, chances for infection. DNA mutation, Thalassemia minor, can be caused by DNA mutation, meaning it is an inherited problem (Mayoclinic, 2020a).
The parents or any one of the parents can transfer thalassemia to the child. The inherited problem of thalassemia minor can stay for a lifetime with a person. Hemoglobin disorder, thalassemia, occurs due to a deformity or disease in hemoglobin (Mayoclinic, 2020a).
The inherited deformed hemoglobin destroys the RBCs of the body. So, deformed hemoglobin is a significant cause of thalassemia minor. The number of mutated genes often depends on the number of mutated genes that the child will have thalassemia or not (Mayoclinic, 2020a).
A child’s increasing number of mutated genes creates chances for thalassemia minor. There is a chance of 25% that heterozygotes parents can transfer thalassemia to the child, 50% chance of being non-symptomatic, and the rest 25% chance of remaining unaffected (Galanello, & Origami, 2020).
The deformity of hemoglobin stays in the human blood cells for a lifetime as thalassemia minor is inherited, but IDA can be completely curable. The impact of thalassemia minor is worldwide, but they are durable and less harmful (Choudhry, 2017). Distinguishing between middle and moderate IDA from thalassemia characteristic can also be diagnosed as a dilemma both the situations tend to share the maximum number of traits (Ullah et al. 2016).
The proper diagnosis amongst the patients suffering from microcytic Anemia is also very significant. It can give a sign for the supplementation of iron to all the patients suffering from IDA (Muñoz et al. 2016). Therefore, to avoid the unnecessary therapy of iron in the carries of thalassemia and prevention from severe and the forms of lethal thalassemia conditions. In the given framework of premarital counseling in the maximum prevalent regions.
Other than the basic complete blood count, the laboratory examinations such as ferritin hemoglobin study (HbA2 and abnormal Hb) along with the DNA evaluation are the main diagnostic limitations for DA, β-thalassemia, respectively. Hence, the regions where the is due to thalassemia are mainly endemic where there are few health care properties; also, these examine might also not be available (Madu & Ughasoro, 2017).
Hence, many simple broadcast indices have been initiated (Kakkar & Sharma, 2020). According to the author, this broadcast will help distinguish between IDA and the characteristics of thalassemia. In recent times, these were also supplemented with many supposedly improvised executing indices. It has been admitted that none of the indexes is 100% specific or 100% sensitive (Kumar et al. 2017).
According to the author, more complex approaches involve the amalgamation of various simple indices, distinguished multivariate study, or the artificial neural channel computation are inadequate to attain excellent specificity and sensitivity. It is also astonishing that the studies showing a comparison of the broadcasted indices have not shown a consistent picture.
The different qualitative indices in a particular analysis might execute low is another analysis (Kabootarizadeh, Jamshidnezhad & Koohmareh, 2019). The main reasons behind these discriminations are not very vivid; the probability of the differences in the regions in thalassemia genotypes and analysis aspects also execute a massive role.
Thalassemia minor is not treated as a severe issue in medical science. This inherited problem occurs due to DNA mutation. The preventive measures of thalassemia minor can be suggested as, Prescribing the patient supplemental Vitamin B, which is also known as folic acid. Folic acid develops red blood cells in the body.
Avoiding excessive intake of iron can help in controlling thalassemia minor. In this case, the doctor’s recommendation should be taken. Eating a healthy diet can be an energy booster. The weakness and dizziness due to thalassemia can be cured by maintaining a healthy and proper diet system.
The patient should take calcium and vitamin D through food to keep the bones strong. Avoiding infection can also help in preventing thalassemia as the problem is prone to infection. So, keeping a distance from sick people can help the patient to avoid the issues of thalassemia.
The full recovery from thalassemia minor in the human body is impossible because it occurs through a genetic transformation, but taking necessary measures can help a patient remain healthy.
Furthermore, the maximum of the published studies comprised a small number of patients, to a few hundred patients only (Hawaldar, Sodani & Arora, 2018). Therefore, this can also explain the outcomes of the variables so that they can easily overcome the numerical bindings. In figure 1, the study with the usage of meta-analysis and the composite of ROC study to compare diagnostic execution and many other distinguishing indices have been showcased.
Figure 2: Different indices for discriminating thalassemia characteristic from iron deficiency anemia amongst the patients with the microcytic RBC
Source: (Hoffmann, Urrechaga & Aguirre, 2015)
The preliminary result in the study was based on the execution of the various makers in the differential diagnosis of the microcytic Anemia as the quantified in respect of the true negative (TN), true positive (TP), false negative (FN), and false-positive (FP) values. All these values are also retrieved from various other sources and have been incorporated into the database.
The study with the specificities and sensitivities of almost 100% [that is, studies with the least zeros in any specific cell (TN, TP, FN, FP)]. Nearly 0.5 analysis is also incorporated into the other four cells for the main purpose of conducting the analysis (Gupta, Nag & Mathur, 2019).
The negative likelihood ratio (NLR) with the 95% of the confidence intervals (95% CI) and the Pooled positive likelihood ratio (PLR) have been calculated by using the random effects of models(Hoffmann, Urrechaga& Aguirre, 2015). The summary of the specificities and sensitivities also has been computed to evaluate the clinical efficacy. However, both broadcasting parameters have not been considered appropriate for the meta-analysis.
According to Hoffmann, Urrechaga& Aguirre (2015), the accurate measure that has been calculated the diagnostic odds ratio (DOR), the sign of the examination accuracy comprising the amalgamation of both specificity and sensitivity. It is also not dependent on any disease prevalence that will ensure its appropriateness for comparing the various studies.
The maximum DOR value is the improvised discriminatory evaluation executed that has been presented in the study. The summary receiver operating characteristic (SROC) curves also have been used to shorten the whole examination performance (Spahn et al. 2019). Therefore, this will help the calculation of the area under the SROC curve (AUC), which is also very vigorous to heterogeneity. The value of AUC <0.75 implies that it has been showcased in the examination to indicate deficiencies in the diagnostic correctness.
Regarding the evaluation of the heterogeneity, the inconsistency index (I2) that enumerates the proper proportion of the whole variation throughout the study that is occurred by the heterogeneity instead of the chance, that would indicate at the I2 value >30% (Hoffmann, Urrechaga & Aguirre, 2015).
The sensitivity study has also been conducted in accordance with the area of the patient’s age, origin (children or adults), and the kind of analyzer. The bivariate generalized linear mixed-effects regression model. Therefore, this model examines the sturdiness of the meta-analytical synopses to compare the outcomes amongst the various distinguished formulas that are evaluated (Urrechaga & Hoffmann, 2017). The bivariate model also accounts for the potential between the study heterogeneity and incorporation of the probable correlation between the FP rate and sensitivity.
According to Hoffmann, Urrechaga& Aguirre (2015), the publication’s bias also has been evaluated by observing and using a scatter plot that is inverse of the square root that is effective of the sample size (1/√ESS), versus the log odds ratio diagnosis. That has a proper and symmetric funnel shape in the publication, and the biasedness was also wholly absent (Matos et al. 2016).
The formal evaluation for the biasedness of the publication was conducted with the usage of a regression of the log DOR that is against 1 ESS along with the weighting in accordance of the effectiveness of the sample size also the weighting it in accordance to the efficacy of the sample size with p<0.10 marking the significant asymmetry (Hoffmann, Urrechaga & Aguirre, 2015).
About 147 results have been recognized in which one of the distinguished indices also have been showcased, and the twelve of the discriminant indices also have been showcased through five or more than that in figures 1 and 2. Altogether, 99 studies have been incorporated 135,409 patient outcomes starting from 3091 for the M/H ratio to almost 22,022 for the England and Fraser index shown in table 2. 30 different discriminant formulas have been investigated in <5 analysis and hence, were exempted from the present meta-analysis (Hoffmann, Urrechaga & Aguirre, 2015).

Figure 3: Twelve distinguished indices validated in five or even more publications.
Source: (Hoffmann, Urrechaga & Aguirre, 2015)
Amongst all the 99 studies, 36 (that is 36%) are mostly from Europe, from the Mediterranean area 24 (that is 24%) (Carla et al. 2020). Southeast Asia, it is 20 (that is 20%), North America 14 (that is 14%), and the remaining analysis was observed from Australia and Latin America. There was almost forty-one analysis (41%) that has been investigating the adults, and 11 (that is 11%) involved only children, and 13 (that is 13%) emphasized on the amalgamated population, which involved both children and adults.
In contrast, 35 (that is 35%) did not mention the age group from which the study was conducted. In regards to the hematology analyzers also used (Hoffmann, Urrechaga & Aguirre, 2015). 32 (that is 32%) of the examination was executed with Coulter, 20 (that is 20%) was conducted with Bayer, and 18 (that is 18%) was conducted through Sysmex. The remaining 30% was performed with different analyzers or different type of analyzer that was not mentioned or specified (Piriyakhuntorn et al. 2018).
Distinguishing IDA from the carrier of thalassemia position is an often issue in the medical practice, specified in many subjects with moderate or mild IDA in the areas where thalassemia is mainly common (Origa, 2017). Therefore, it is impossible to differentiate both the situations that are by the usage of the simple blood counts because both of them are interlinked with the hypochromic erythrocytes and microcytic (Shiang Yui et al. 2020).
Furthermore, in thalassemia, RBC tends to be very microcytic, whereas the deficiency of iron that is RBC are more often hypochromic (Lei et al. 2019). Therefore, all these distinguished have been oppressed by the simple growing formulas of mathematics to emphasize the various RBC index as a medium for differentiating IDA from the characteristic of thalassemia (Hoffmann & Urrechaga, 2020).
Furthermore, the distinguished authority of the simple index has not been able to acquire the diagnostic presentation. The considerable amount of distinguished index elaborated in the study also states that the research has been executed based on the local patients considering them to sample and conducting the study accordingly (Hoffmann, Urrechaga & Aguirre, 2016).
A meta-analysis also has certain inherited limitations that also instigate issues while conducting a study, especially the problems that arise in the methodological process. The designs that are selected for the study are also properly investigated that are any from homogeneous; also, there has been a variation in the selection of patients in the kind of hematology analyzer used but in cut-off value for the respective distinguished index (Amalia, 2020). In particular, all these aspects play a significant role in the utility of the diagnosis of the index (Laengsri et al. 2019).
Iron deficiency anemia can be treated with the advice of a proper physician, doctor, or nutritionist. The problem needed to be cured by giving iron supplements to the patient. By taking regular iron tablets on an empty stomach, a patient can increase the iron level in the blood, which will help in developing RBC, and the oxygen supply will remain uninterrupted. Vitamin C absorbs iron in the cells and provides enough iron to create RBC (Mayoclinic, 2020b).
So, iron tablets can be taken with vitamin C. Doctors often suggest it. Antacid can stop iron absorption (Mayoclinic, 2020b). It is needed to take iron tablets and antacids with a minimum interval of time. The vegetarians who do not eat meat cannot supply enough iron to their bodies. A proper nutritionist can suggest a proper diet to the vegetarians for taking supplemental iron. The woman who suffers from excessive menstrual bleeding needs blood transfusion so that the lack of iron can be fulfilled, and it can create RBC for oxygen supply.
Blood transfusion is a temporary solution. The patient should take preventive measures for long term health security. This process is used to provide iron to the blood cells. It takes a few sessions to replenish the amount of iron in the patient’s body (NHLBI, 2020). Patients who have severe iron deficiency often go for iron therapy. Other treatment processes include surgery such as endoscopy for stopping extra bleeding, iron-rich food intake, and drinking black tea (NHLBI, 2020).
There are various types of thalassemia out of which maximum study tends to emphasize the carriers of the β-thalassemia. Few studies also tend to focus on both carriers of α β-thalassemia (Roth et al. 2018). Certain studies have been focusing on the carries of the α-thalassemia and α- and δβ-thalassemia.
The entire picture states that the emergence from all the above studies and the distinguished index also tends to execute better in β- rather than in α-thalassemia. Even though microcytic carriers of α-thalassemia are included (Çil, Ayyıldız & Tuncer, 2020). Therefore, IDA in the thalassemia carrier also has no means that has a rare finding, and many analyses also involved individual patients that are most likely to have IDA (İndeksler, 2019).
The study has been showcasing all the evaluations related to the patients suffering from thalassemia. The microcytic Anemia that occurs because of iron-deficiency Anemia (IDA) is most common in all countries. The journals were reviewed to find the proper explanation and differences amongst the various types of thalassemia.
A considerable number of accurate analysis among the patients suffering from microcytic Anemia is also significant. It can give a symbol for the subjunction of iron to all the patients suffering from IDA. The study involves numeric representation for the Mediterranean regions, the Middle East, Southeast Asia, North America, Europe, and Latin America.
The report states the number of patients suffering from IDA with the traits of thalassemia. The study also shows the tool used to measure RBC indices from the thalassemia characteristic. The different types of thalassemia have also been introduced as the most common one prevalent amongst the patients and the percentage of the prevalent disease.
The gap in the present literature is that the data that has been collected is from various countries, due to which the calculation and the data collected has expanded a lot. Therefore, the data should have been collected from a single country to understand the status in detail.
In contrast, the data expansion fails to provide proper count and positions with an approximate numeric representation. Hence, focusing on a particular country would have helped in conducting an in-depth analysis of that specific country, after which proper measures could have been taken to mitigate them.
Hypothetical statements are given based on assumptions by evaluating the points of argument. It can be of three different forms such as null hypothesis, negative hypothesis, and positive hypothesis. In this case, some hypothetical assumptions can be stated.
H1: The influence of discriminant indices in distinguishing anemia and thalassemia minor.
H2: The role of iron deficiency in formulating Anemia.
H3: The role of iron deficiency in formulating thalassemia minor.
H3: The impact of discriminant indices in treating anemia and thalassemia minor.
The critical evaluation of the discriminant indices to distinguish between iron deficiency anemia and thalassemia minor helps give the idea regarding the impacts of both on human health and which one is more harmful to health. The causes and symptoms of both diseases are stated to give the readers an overview of iron deficiency anemia and thalassemia minor. For both the problems, several treatment procedures are given so that the preventive measure can help the sufferers to relieve.
Moreover, the research paper offers an argumentative study to better explore the topics relevant to the research and the impact them on human health. The arguments from different scholarly sources help the research paper to match its standard with acknowledgeable research papers.
Not only that, through driving information from various academic sources, the researcher gives the reader to have a wide range of knowledge regarding the topic. The formulation of hypothetical statements helps in giving assumptions regarding the research. The research questions provide an overview and clear out the objective or aim of the research. The analysis will also help the researcher expand knowledge and use this research evaluation in the future during the experiment on medical sciences.
Amalia, Y. (2020). Difference of Het Re Level In Thalassemia β Minor And Iron Deficiency Anemia. STRADA Jurnal Ilmiah Kesehatan, 9(2), 1635-1641.
Arora, S., Rana, D., Kolte, S., Dawson, L., & Dhawan, I. (2018). Validation of new indices for differentiation between iron deficiency anemia and beta-thalassemia trait, a study in pregnant females. Int J Sci Rep, 4(2), 26-30.
Braunstein, E. (2020). Overview of Anemia – Blood Disorders – MSD Manual Consumer Version. Retrieved 29 December 2020, from https://www.msdmanuals.com/en-in/home/blood-disorders/anemia/overview-of-anemia
Carla, M. G., Rafael, S. P., Isabel, F. G., Cristina, G. F., & Teresa, S. M. (2020). New haematologic score to discriminate beta thalassemia trait from iron deficiency anaemia in a Spanish Mediterranean region. Clinica Chimica Acta.
Choudhry, V. P. (2017). Thalassemia minor and major: current management. The Indian Journal of Pediatrics, 84(8), 607-611.
Çil, B., Ayyıldız, H., & Tuncer, T. (2020). Discrimination of β-thalassemia and iron deficiency anemia through extreme learning machine and regularised extreme learning machine-based decision support system. Medical Hypotheses, 138, 109611.
DeLoughery, T. G. (2017). Iron deficiency anemia. Medical Clinics, 101(2), 319-332.
Galanello, R., & Origa, R. (2020). Beta-thalassemia. Orphanet Journal Of Rare Diseases, 5. DOI: 10.1186/1750-1172-5-11
Gupta, P., Nag, B. P., & Mathur, A. (2019) Evaluation of Red Cell Indices and Discriminant Functions in the Detection of Beta Thalassemia Trait.
Hawaldar, R., Sodani, S., & Arora, M. K. (2018) Study of discriminant factor M/H ratio in screening for β thalassemia trait.
Hoffmann, J. J., & Urrechaga, E. (2020). Verification of 20 mathematical formulas for discriminating between iron deficiency anemia and thalassemia trait in microcytic Anemia. Laboratory Medicine, 51(6), 628-634.
Hoffmann, J. J., Urrechaga, E., & Aguirre, U. (2015) . Discriminant indices for distinguishing thalassemia and iron deficiency in patients with microcytic Anemia: a meta-analysis, Clinical Chemistry and Laboratory Medicine (CCLM), 53(12), 1883-1894. DOI: https://doi.org/10.1515/cclm-2015-0179
Holm, G. (2020). Everything You Need to Know About Thalassemia. Retrieved 29 December 2020, from https://www.healthline.com/health/thalassemia
İndeksler, A. K. H. (2019). Iron Deficiency Anemia and β-Thalassemia Minor Differentiation With Hematological Indices.
Jahangiri, M., Rahim, F., Saki Malehi, A., Pezeshki, S. M. S., & Ebrahimi, M. (2019). Differential Diagnosis of Microcytic Anemia, Thalassemia or Iron Deficiency Anemia: A Diagnostic Test Accuracy Meta-Analysis. Modern Medical Laboratory Journal, 3(1), 1-14.
Kabootarizadeh, L., Jamshidnezhad, A., & Koohmareh, Z. (2019). Differential diagnosis of iron-deficiency anemia from β-thalassemia trait using an intelligent model in comparison with discriminant indexes. Acta Informatica Medica, 27(2), 78.
Kakkar, N., & Sharma, A. (2020). Discriminant Indices for Screening Beta Thalassemia Trait: An Illusion of Choice. Indian Journal of Hematology and Blood Transfusion, 1-2.
Kumar, A., Saha, D., Kini, J., Murali, N., Chakraborti, S., & Adiga, D. (2017). The role of discriminant functions in screening beta thalassemia trait and iron deficiency anemia among laboratory samples. Journal of laboratory physicians, 9(3), 195.
Laengsri, V., Shoombuatong, W., Adirojananon, W., Nantasenamart, C., Prachayasittikul, V., & Nuchnoi, P. (2019). Thai red: a web-based prediction tool for discriminating thalassemia trait and iron deficiency anemia. BMC medical informatics and decision making, 19(1), 212.
Lei, M. Q., Sun, L. F., Luo, X. S., Yang, X. Y., Yu, F., Chen, X. X., & Wang, Z. M. (2019). Distinguishing iron deficiency anemia from thalassemia by the red blood cell lifespan with a simple CO breath test: A pilot study. Journal of breath research, 13(2), 026007.
Madu, A. J., & Ughasoro, M. D. (2017). Anaemia of chronic disease: an in-depth review. Medical Principles and Practice, 26(1), 1-9.
Matos, J. F., Dusse, L., Borges, K. B., de Castro, R. L., Coura-Vital, W., & Carvalho, M. D. G. (2016). A new index to discriminate between iron deficiency anemia and thalassemia trait. Revista brasileira de hematologia e hemoterapia, 38(3), 214-219.
Muñoz, M., Acheson, A. G., Auerbach, M., Besser, M., Haber, O., Kehlet, H., … & Richards, T. (2017). International consensus statement on the peri‐operative management of anaemia and iron deficiency. Anaesthesia, 72(2), 233-247.
NHLBI. (2020). Iron-Deficiency Anemia. Retrieved 29 December 2020, from https://www.nhlbi.nih.gov/health-topics/iron-deficiency-anemia
Origa, R. (2017). β-Thalassemia. Genetics in Medicine, 19(6), 609-619.
Piriyakhuntorn, P., Tantiworawit, A., Rattanathammethee, T., Chai-Adisaksopha, C., Rattarittamrong, E., & Norasetthada, L. (2018).
The role of red cell distribution width in the differential diagnosis of iron deficiency anemia and non-transfusiondependent thalassemia patients. Hematology Reports, 10(3).
Roth, I. L., Lachover, B., Koren, G., Levin, C., Zalman, L., & Koren, A. (2018). Detection of β-thalassemia carriers by red cell parameters obtained from automatic counters using mathematical formulas. Mediterranean journal of hematology and infectious diseases, 10(1).
Shiang Yui, W. E. E., Said, S. S. M., Sabudin, R. Z. A. R., Alauddin, H., & Ithnin, A. (2020). Microcytic to hypochromic ratio as a discriminant index of thalassaemia trait in subjects with hypochromic anaemia. Malays J Pathol, 42(2), 195-201.
Spahn, D. R., Schoenrath, F., Spahn, G. H., Seifert, B., Stein, P., Theusinger, O. M., … & Falk, V. (2019). Effect of ultra-short-term treatment of patients with iron deficiency or anaemia undergoing cardiac surgery: a prospective randomised trial. The Lancet, 393(10187), 2201-2212.
Transfusion, (2020). Retrieved 29 December 2020, from https://transfusion.com.au/sites/default/files/07%20LRI%20Spectrum%20of%20iron%20deficiency%20without%20header%20-%20900%20px%20wide.png
Ullah, Z., Khattak, A. A., Ali, S. A., Hussain, J., Noor, B., Bano, R., & Mahsud, M. A. J. (2016). Evaluation of five discriminating indexes to distinguish Beta-Thalassemia Trait from Iron Deficiency Anaemia. J. Pak. Med. Assoc, 66(12), 1627-1631.
Urrechaga, E., & Hoffmann, J. J. (2017). Critical appraisal of discriminant formulas for distinguishing thalassemia from iron deficiency in patients with microcytic Anemia. Clinical Chemistry and Laboratory Medicine (CCLM), 55(10), 1582-1591.
Gotter, A. (2021). Everything You Need to Know About Microcytic Anemia. Retrieved 4 January 2021, from https://www.healthline.com/health/microcytic-anemia
Hematology,(2021) Iron-Deficiency Anemia. Retrieved 4 January 2021, from https://www.hematology.org/education/patients/anemia/iron-deficiency
Common symptoms of iron deficiency include fatigue, weakness, pale skin, shortness of breath, dizziness, headache, cold hands and feet, brittle nails, and restless leg syndrome.
You May Also Like
All work is written by human writers. 100% AI free, guaranteed.
100% money back guarantee if you find plagiarism in our work.
COMPANY DETAILS