Here is a sample that showcases why we are one of the world’s leading academic writing firms. This assignment was created by one of our UK literature review writers and demonstrated the highest academic quality. Place your order today to achieve academic greatness.
Table of Contents
Nitrogen dioxide (NO2), is a kind of gas generated by in fuel burning stoves. However, it is also emitted by automobile engines, cigarette smoke and coal-burning plants (EPA, 2016). Studies on the effect of NO2 on the body included damaging of epithelial cells (World Health Organization, 2006). There are several studies on the harmful effects of nitrogen dioxide on the health. Although there are no studies showing a specific concentration that affect our health, the relationship between an increase in inhalation of nitrogen dioxide and its effect on health is still poorly understood (Oda et al., 1981).
Nitrogen is a natural inorganic element that is formed by 78% of the earth atmosphere molecules. It can be found in the human body, e.g. nucleotides and hormones.
Nitric oxide (NO) plays an important role in living organisms and in physiological and pathological processes, acting as a second messenger in the cells and playing various crucial roles within the body, such as endothelium-dependent dilation, angiogenesis and leukocyte adhesion.
NO bioavailability has two directions; it is delivered as a form of gas which diffuses across the membrane barriers (alveolar and endothelial), leading to an increase in cGMP which in turn increases muscle relaxation and vasodilatation. However, in the presence of oxygen, it is converted into toxic molecule which is nitrogen dioxide (NO2). (Figure. 1) (Hayward, 1999).
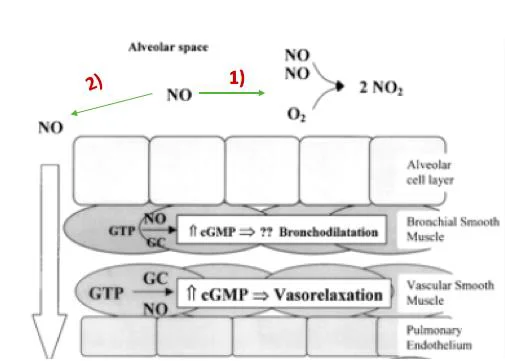
Figure 1. The directions of gas nitric oxide that has been inhaled. 1) shows the conversion of nitric oxide to toxic gas, which is the nitrogen dioxide. 2) diffusion of NO via membrane and its role in vasodilation (Hayward, 1999
NO is a is produced in the endothelial cells by utilising amino acid L-arginine via an enzyme called nitric oxide synthase (eNOS) (Fig. 2) (Furchgott and Zawadzki, 1980).
NO reacts with haemoglobin to form S-nitrosohemoglobin (SNO-Hb). Haemoglobin acts as a transporter to transfer nitric oxide and oxygen to the peripheral areas where oxygen and nitric oxide is required (Cannon et al., 2001).
Nitrite and nitrate were previously considered inert biologically and end product of nitric oxide. However, currently recent studies found that these inert anions can be used as an important alternative stock of nitric oxide in humans (Lundberg et al., 2008).
In addition, the concentration of nitrate in the plasma is usually 30uM while nitrite is relatively less (Langrish et al., 2013). According to a study conducted by Oda et al., (1981) it was found that, after exposing mice to gas of nitrogen dioxide the rate of nitrite in the blood was increased with longer half-life (Oda et al., 1981).
With regards of nitrate, green vegetables are considered as a source of systemic nitrate, boosting nitrate-nitrite-NO pathway (Khatri et al., 2016; Mills et al., 2016). Numerous studies have demonstrated the benefits of dietary nitrate to prevent cardiovascular disease and certain type of cancers (Khatri et al., 2016). However, the effect of inhaled nitrogen dioxide on nitrate-nitrite-NO pathway is unknown.
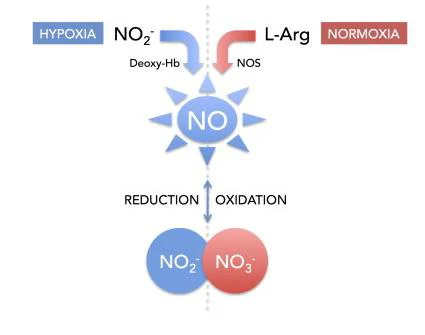
Figure.2 In normal level of oxygen, the nitric oxide is produced through the L-arginine via an enzyme called nitric oxide NO synthase (eNOS). While in case of absence oxygen, production of nitric oxide from reduction of nitrite by deoxyhemoglobin
Endothelium is a layer of thin cells that is found in the internal cavity of the blood vessels (inner lumen), responding to the chemical and mechanical stimuli, helping in the regulation of vascular tone, inflammation response and thrombosis (Deanfield et al., 2018).
Any dysfunction in the endothelial cells may lead to development of atherosclerosis as a result of impaired vasodilation and increased of thrombotic state (Giles et al., 2018).
According to American Heart Association (AHA), an increase in exposure to particulate matter (PM) led to an increase of cardiovascular disease, contributing to the mortality and morbidity (Brook et al., 2010). It has also been shown that the rate of impaired endothelial function resulting from exposure to particulate matter such as diesel exhaust (DE) may play a significant role in vascular and fibrinolytic dysfunction.
However, regular exercise was found to reduce this development to prevent cardiovascular diseases development (Warburton, 2006). Nevertheless, a different study found that during the exercises increases breathing and thus increases the doses of pollutants that are inhaled and this led to increase air pollution adverse effects more than exposure during rest (Daigle et al., 2003).
There are no sufficient researches on how pollutants affect endothelial functions (Bräuner et al., 2008; Wauters et al., 2013). For example, some studies have suggested that exposure to pollutants, especially during exercise, increases health problems such as reduced vascular functions and increased pulmonary artery pressure (Rundell et al., 2010).
Conversely, other studies have indicated that exposure to PM or DE does not cause vascular dysfunction either with or without excercise, but this imbalance also exists in individuals who are not physically active (Wauters et al., 2013). Moreover, there is no study explaining how exercise changes physiological response when exposed to PM (Giles et al., 2018).
However, nitric oxide is rapidly convert to nitrogen dioxide by atmospheric oxidation factors such as oxygen (Jarvis et al., 2018). Studies have demonstrated the change in nitric oxide level after exposure to DE as a result of endothelial dysfunction (Nurkiewicz et al., 2009). Although other studies have shown that exposure to nitrogen dioxied which is the main component of PM is the causative of cardiovascular diseases.
In contrast, there are study has found that after controlling the exposure to DE the problems of vascular disorder still exist. Moreover, According to Langrish et al. (2010) these side effects caused by exposure to pollutants may be caused by other fine and ultrafine particulate matter rather than nitrogen dioxide and other gaseous.
Besides, different study demonstrated that the nitrogen dioxide is insoluble therefore cannot reach to bloodstream via lungs (Postlethwalt., 1991). Some researchers have suggested that an increase in the level of nitric oxide in mice after exposure to DE and this can be used to regulate the production of vasculer nitric oxide . Also, recent studies reported that the level of nitric oxide- end products increased in blood circulation after exposure to DE (Knuckles et al., 2011).
Nitric oxide-dependent signalling pathway, forming via protein S-nitrosation, is involved in almost all biological process of cell, from proliferation, to homeostasis, to programmed cell death as well as immunity and vascular tone (Broniowska and Hogg, 2012).
Since nitric oxide (•NO) has a short half-life, it is preserved via S-nitrosation reactions, forming a buffer carrier and donor proteins known as S-nitrosothiols (RSNOs) (Gaucher et al., 2012). These proteins (RSNOs) are biologically-relevant products of NO and have been recognised as indicators since NO cannot be detected per se in the plasma (Diers, Keszler and Hogg, 2014).
In order to understand the contribution inhaled NO2 and the Nitrate–Nitrite–Nitric Oxide Pathway, one has to understand about toxicokinetics and metabolism of NO2.
However, due to the nature of scientific challenges involved in researching in this area, there are very limited amount of publications on kinetics and metabolism of NO2.
Furthermore, most of the available data in this direction limited to the deposition and fate of NO2 in the victim’s respiratory tract. Accordingly, mathematical modelling research indicate that the placement of NO2 in the tissues of the lower respiratory tract is thought to be optimal at intersection of the conducting airways and the NO2 exchange area within human lungs (Overton, 1984).
According to Chitano et al., (1995), the health impacts of inhaled NO2, in most of the lung biochemical studies report that the effects depend on the length of exposure. However the same authors cited that a notable exception was the effect of the NO2 on the metabolism of the lung lipid.
For instance, exposure of rats to indoor NO2 was found to escalate lipid peroxidation in small amount (as low as 700 μg/m3). In a study done by Ichinose and Sagai, (1982), found that the effects of NO2 on both lipid breakdown and antioxidant absorption reported a response pattern that was dependent upon both concentration levels and length of exposure to the gas.
One of the common features of elevated levels of NO2 includes lung edema couple with an increased antioxidant breakdown. However these changes even though still not fully understood, could be attributed to cell lesions.
Concentrations more than 2000 μg/m3 are essential during acute managed exposures to cause alterations in pulmonary role in healthy human beings(Ichinose and Sagai, 1982; Berglund, 1993).
Due to the fact that these concentrations do not exist in usual air, studies in regards to the effects of NO2 has been narrowed to individuals suffering from lung complications.
Furthermore, there have been several publications on patients with asthma, pulmonary illness, and chronic bronchitis indicating that exposure to reduced concentrations of indoors NO2 can result in small reductions in vital capacity and expiratory volume (WHO, 2000).
Accordingly, Linn et al., (1986) in their study did not find pulmonary feature responses at concentrations between 1880–7520 -μg/m3. In fact even within the same lab location, their findings have never be reproduced with various samples of asthmatic patients (Roger et al., 1990).
In a different study conducted by WHO, (2000), it was discovered that minimal exposures to NO2 levels of 1.6 ppm resulted in increased airway obstruction in patients suffering from obstructive pulmonary illness. However at similar concentrations in individuals exercising moderately for 1 hour, no responses were observed (WHO, 2000).
Thus longer exposures to NO2 have been thought to cause functional problems in people with obstructive pulmonary complications at lower concentration.
Nevertheless, the explanations for the kind of mixed findings are still vague even though it has been believed that inhalation of indoor NO2 escalates the airway resistance at normal concentrations.
Another possible explanation for this observation could factor in the variation in methodology and sample selection technique. Other studies have reported similar albeit statistically non-significant results in relation to the effects of indoor NO2, however, this suggest that caution needs to factored in when sanctioning these kind of findings to avoid some sorts of conflict.
Professional editors proofread and edit your paper by focusing on:
Studies on indoor exposure to NO2 studies have been carried out in the context of the gas combustion gases in a gas cooker (WHO, 2000). However, the studies conducted on adults have failed to show the link between the utilization of gas for cooking purposed and respiratory or lung functions.
Even though an epidemiological research carried out on elderly female using gas cookers indicated an increase in the incidences of asthma signs and impaired breathing, Jedrychowski et al., (1995) reported that there are no meaningful changes in FEV1 and FVC data.
Albeit there could be exceptions, most of lung biochemical publications report impacts only following acute or exposure to NO2 concentrations exceeding 2 ppm (Berglund, 1993).
Nevertheless, an exception worth noting is the impact on the metabolism of lung lipid. For instance, in a study done by Jarvis et al., (2010) it was found that the exposure of rats to gas cooker NO2 elevates lipid peroxidation at minimal concentrations (as low as 0.4 ppm).
Never at elevated levels, had ethane levels had normalized after 28-month period. Impact on both lipid and antioxidant breakdown indicated a response behaviour that relies on both NO2 levels and length of exposure (Sagai, Ichinose and Kubota, 1984).
Regularly reported features at elevated NO2 concentrations entail the oedema of the lungs, an optimized antioxidant absorption, an elevation in the level of lung enzymes relayed with cell damage, lung lipid structure alterations. Consequently, these changes, albeit still not fully known, is suspected to be suggestive of early symptoms of cell lesions.
On the other hand, several epidemiological reports have indicated relationship between livings in house with cooking gas stoves and high incidences of respiratory problems especially among toddlers (WHO, 2000). Respiratory disease is a generic phrase used to refer to indications gathered in various epidemiological inquests, for instance, chest congestion, wheezing sounds, cough and asthma.
However, the evidence varies based of different studies and this makes it challenging to making valid conclusions in this area. Lin, Brunekreef and Gehring, (2013) carried out comparative studies in households that cooked using gas stoves. Based on the findings of the study, the authors noted presence of lower respiratory complications in kids aged 6- 10 years.
This study is a part of a research being conducted by Dr Webb and his team, aiming to assess the effect of nitrogen dioxide found in gas cooking on nitrate-nitrite-NO pathway and cardiovascular function. Exposure to nitrogen dioxide is thought to be harmful to the body, causing cardiovascular and respiratory diseases.
However, the potential effect of indoor exposure to nitrogen dioxide on the rate of nitrate-nitrite-NO has not been investigated. This effect could boost the NO production which has a central role in vasodilation and thus reducing the risk of developing hypertension and cardiovascular events.
Therefore, the main aim of this study is to investigate whether the indoor exposure to nitrogen dioxide found in gas-cooker affects nitrate-nitrite-NO pathway, boosting the NO production. Our hypothesis is that the exposure to nitrogen dioxide has no effects on nitrate-nitrite-NO pathway and thus NO production.
At the beginning, healthy volunteers were recruited after responding to advertisements and e-mails by King’s College London Research Volunteer recruitment fortnightly circular. Participant Information Sheet (PIS) was sent to the interested volunteers which explained the principles of the study.
After that, the approval paper was taken after the participant met the required criteria, including, 18-45 years of age, body mass index (18-40kg/m2), SBP 90-140mmHg and DBP <90mmHg of normotensive. Participants were required to avoid over-the-counter medications (except oral contraceptive drugs) as well as vitamins or herbal supplements.
Also, they were expected not to have had s recent history of infection or any other illness. With regards female participants, they were expected not to be pregnant or planning to be pregnant during the study. Participants who underwent the experiment were required to abstain from eating or drinking 12 hours before commencing the study and only water was be given during the session.
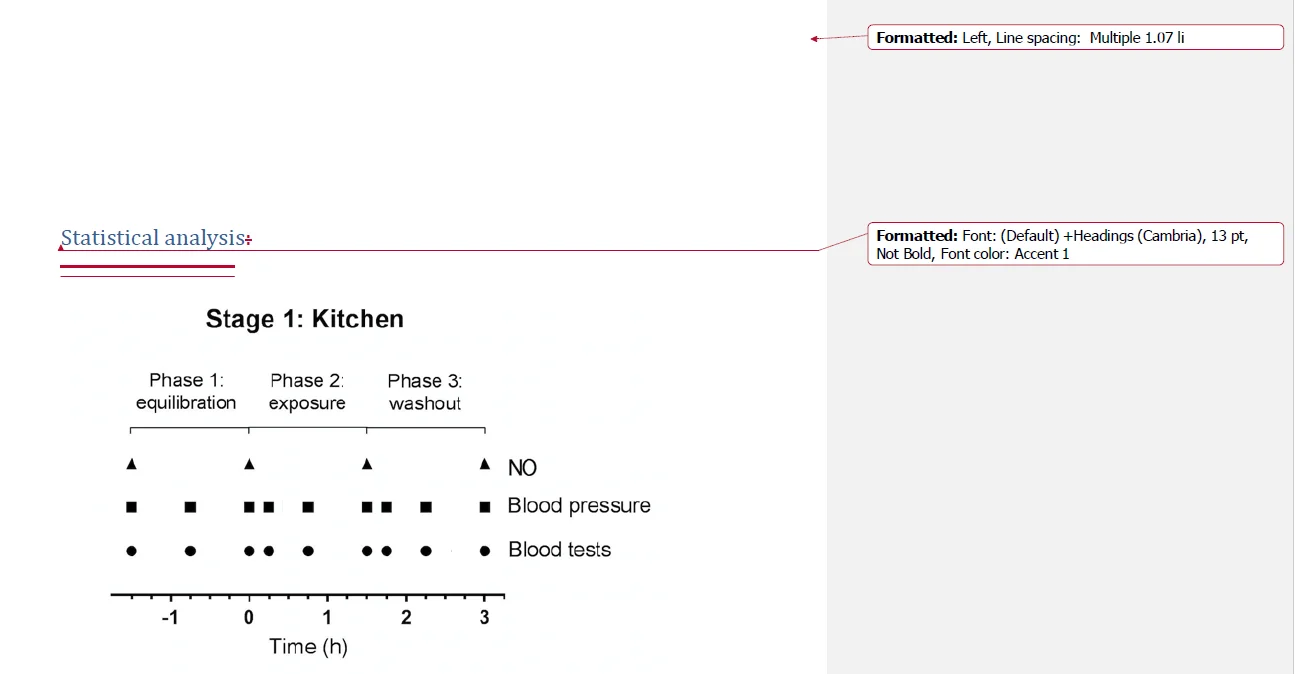
The study was approved ethically by the Local Research Ethics Committee. It was open-label, single-centre, randomised, paired, crossover study, including # healthy participants. Each participant was undergone two visits, control and kitchen. During the control visit, participants were restrained from inhaling cooking-gas in resting room, whereas in the kitchen visit, they were exposed to cooking-gas for 90 min.
This was undertaken to compare the potential impact of inhaled nitrogen dioxide on plasma nitrate- nitrite-NO, and subsequently associated biological responses. The blood samples (8ml) and blood pressure were taken every 45 min over three stages, pre-exposure (three samples), exposure (three samples), and post-exposure (three samples).
All volunteers were asked to fast for 12 hours before starting the study day. During 24 before the start of the experiment, the volunteers were also asked to avoid foods containing high-nitrate (they were given a list of all foods containing nitrate), caffeine, smoking and strenuous exercise.
To avoid confusion during the study days, the volunteers were given a diary containing the food and drink they could eat at 24 hours before the study day to ensure that all volunteers have the same food.
The volunteers were invited for two visits to the MRU at Franklin- Wilkins building with a gap of less than 7 days between two visits. Each visit was approximately 4.30 hours (90 minutes before exposure, 90 minutes during exposure and 90 minutes after exposure).
The measurements were taken in order, starting with taking the blood pressure, measuring exhaled NO and collecting the blood samples (similar manner in both visits).
The difference between two visits, which depended on randomisation was to stay in the resting room (control) or exposure to nitrogen dioxide through the gas-cooker (kitchen). Eating and drinking was controlled during study day, only still water (250ml) was drunk before and after measurement of exhaled NO (buxton mineral water used because it has low nitrate content).
Medical information was collected which included dhistory of diseases such as cardiovascular disease or any family members have diabetes. Also, the researcher collected the number of times smoking or drinking alcohol. Before commencing the study, background nitrate concentration was measured (by using the NO breath FeNO)
According to British Hypertension Society guidelines, Omron 705IT (Omron Corp., Tokyo, Japan) was used to measure blood pressure(BP) and heart rate(HR) (Williams et al., 2004). In terms of baseline, Blood pressure readings were taken triplicates every 45 minutes, pre- exposure to the gas oven (-1.30h, -45min and 0), during exposure (15 min, 45min and 1.30) and after exposure (1.45h,2.15h and 3)(image2).
For the first set of measurements, blood pressure was measured in both arms, while for the rest of the study, one arm was selected depending on the comfort of the volunteers. The temperature of the room was also recorded with a pressure measurement (about one meter away from the volunteer) by using temperature probe. Volunteers were prevented to moving or speaking during BP measurement.
After measuring the blood pressure, 10 ml of the blood samples were taken by prechilled syringe and then transferred to 8 ml prechilled sodium-heparin Vacutainers through standard venepuncture and using of the butterfly needle , which was remaining in the arm until the last sample(except if it stops had to be taken again).
After that, Hettich Mikro 220R centrifuge (Sigma-Aldrich Company) was used (4500g, 4C for 5mins) to separate plasma. Samples were collected before exposure to gas cooker burning (-1.30h, -45min and 0), and during exposure (15 min, 45min and 1.30) also after exposure (1.45h,2.15h and 3)(Figure 2).
A pipette was used to separate the plasma and transfer it to three pre-labelled aliquots. The aliquots were kept in boxes and stored initially in freezer(-80 ° C) before transferred to Thomas hospital to analyse the concentration of nitrite, nitrate and nitrosothiol.
Exhaled NO recording NO breath Kit FENO monitor (Bedfont Scientific Ltd) measuring device was used for measuring exhaled NO (eNO).
Before the measurements, volunteers were explained how can use this equipment. Before exposure to gas (equilibrium phase) exhaled NO was measured twice at-1.45h -45min and 0h by taking readings two times (before drinking water and after drinking water (250mls Buxton water). After exposure, exhaled NO was measured similarly by same equipment after 1.5hour from the onset of exposure and similarly in post-exposure (3h).
To analyse nitrite concentration in plasma was used Ozone-based Chemiluminescence assay was carried out using the 280i Nitric Oxide Analyser (NOA) (Sievers Instruments, GE analytic instruments).
All the procedures in laboratory were carried out under the supervision of an experienced laboratory technician or the manager of CRF. At the begging, a standard curve was obtained by using different concentrations of sodium nitrite (10mM, 1mM, 100μM, 10μM, 5μM, 2.5μm, 1.25μM, 1μM, 0.5μM, 0.25μM and 0.125μM).
Then, 0.5g of sodium iodide and 45ml of lactic acid were diluted in 5 ml of water to prepare reducing reagent iodide. The samples were analysed if standard curve is appropriate (R2~1, -100 ≤intercept ≤ 100). The plasma was then analysed without dilution to determine nitrite concentration.
Nitrogen dioxide is not commonly used in medicine due to its toxic nature. It is an air pollutant and exposure can cause respiratory problems. However, nitrogen oxide compounds may have limited applications in the treatment of certain diseases, such as pulmonary hypertension, but further research is needed.
You May Also Like
All work is written by human writers. 100% AI free, guaranteed.
100% money back guarantee if you find plagiarism in our work.
COMPANY DETAILS