Here is a sample that showcases why we are one of the world’s leading academic writing firms. This assignment was created by one of our expert academic writers and demonstrated the highest academic quality. Place your order today to achieve academic greatness.
Table of Contents
The ratio of elderly patients in the general population is increasing steadily in Western countries. According to Fazel, Geddes, and Kushel (2014), elder people are highly diversified with great differences within the general health state, frequently with several coexisting diseases. Regarding this, elderly people have higher chances of increased length of post-operative stay and rate of readmissions after surgery.
Gastric cancer has been the third major cause of morbidity and mortality and the fourth most common type of cancer across the world, particularly in South America, Central, and Eastern Europe, and Eastern Asia. Recently, several different interventional strategies or measures have been implemented during the perioperative care of colorectal and gastric cancer that facilitate patients’ recovery, such as gastrectomy with lymphadenectomy. This is perioperative chemoradiotherapy that is administered increasingly in elder patients with advanced diseases like gastric or colorectal, promoting patient recovery.
However, Jia et al. (2014) stated that the morbidity rate after gastrectomy had been reported to 13.8-46.0% and poses a considerable financial strain on patients, families, and healthcare facilities due to increased readmission cases increased length of hospital stay at the hospitals.
In this regard, there is a need to reduce the length of hospital stay within the post-operative care and readmission cases with significant and effective post-operative recovery intervention to enhance patient recovery after surgery and reduce readmission rate and length of stay at hospitals.
Taking into consideration, Wang et al. (2011) emphasised that the Enhanced Recovery After Surgery (ERAS) is a standardised pathway or protocol that has extensively been implemented for attaining significant improvements in reducing post-operative length of stay at hospitals. ERAS is also termed as Fast Track Protocol which Henrik Kehlet developed in 1994. Over the last few decades, this technique has been used increasingly due to having vast applications and significant safety and benefits.
Moreover, Shida et al. (2015) stated that ERAS is a multidisciplinary approach determining to decrease stress response after surgery and facilitate reduced length of hospital stay and allow reduced complication rate followed by surgery, including gastric or colorectal surgery.
In addition to this, according to Pędziwiatr et al. (2016), ERAS pathway has considered as a care standard and proven to be effective and beneficial for patients after colorectal surgery or gastric surgery. ERAS pathway intends to reduce length of stay and post-operative stress at reduced costs.
During perioperative period, patients are educated on the ERAS pathway and given written instructions, along with informational pamphlet that include programme briefing with a focus on improving mobility and stability. However, there is a concern regarding the applicability of ERAS pathway to the elderly population and requires an active participation from elder patients after their gastric or colorectal surgery.
Furthermore, Bona, et al. (2014) stated that the ERAS pathway protocol contains several essential components. It is uncertain which of these variables or components contribute significantly to increased recovery after surgery, particularly amongst the elder population.
Thus, the following research is based on systematic literature review that intends to critically analyse the outcomes of ERAS strategy or pathway in elderly patients that have gone through gastric or colorectal surgery with reduced length of post-operative stay at hospitals and rate of readmissions amongst elder patients.
Previous studies and published reports have reported a wide adoption of ERAS protocol in Europe. However, in countries where resources and healthcare management are decentralised, the implementation of ERAS is facing substantial challenges. It poses a threat to ERAS protocol’s efficacy in declining the length of post-operative stay among elderly patients.
Moreover, Sugisawa et al. (2016) stated that several previous prospective researches have reported the feasibility and efficacy of ERAS pathway for gastric and colorectal cancers and have found safe indications. However, few of the studies reported less feasibility of ERAS protocol and unsuccessful implementation of ERAS pathway among elderly patients with gastric or colorectal cancer that may lead to the financial strain of patients and their families, along with hospitals about enhanced length of stay at hospital and readmission cases within the healthcare facility.
In this regard, the following study determined to analyse the feasibility of ERAS protocol for reducing length of post-operative stay and readmissions rate in gastric/colorectal elderly patients based on reviewing previous prospective studies.
In the following study, the researcher aims to conduct a systematic literature review to analyse to what extent ERAS protocol is useful for reducing readmission cases and length of stay after surgery, particularly in elderly patients with gastric or colorectal cancer. Following secondary objectives have also been formulated to achieve main aim of the study:
Research question of the following study is:
The rationale behind conducting this research is to increase awareness regarding the usefulness of ERAS programme in lowering the readmission rates and post-operative length of stay demonstrated in recent prospective studies after implementing enhanced recovery pathways in gastric/colorectal elderly patients.
The present study has high public health significance as patients and healthcare systems are facing financial strain as a result of increased post-operative length of stay and readmission cases followed by gastric or colorectal surgery that can be reduced through adopting recommendations outlined in the study and successfully implement the ERAS programme for reducing length of stay at hospitals and rate of readmissions in gastric or colorectal elderly patients as well reducing financial burden of additional costs caused by complications after gastric or colorectal surgery.
In the words of Muller et al. (2009), there have been marked differences found in the results of length of stay across individual studies and reviews that reflect differences in ERAS programmes, healthcare management and procedures, compliance to ERAS protocols, and outcome definitions particularly in elderly patients. This has raised concerns regarding the impact of ERAS programmes on post-operative length of stay and rate of readmissions, which are overstated in some studies and reviews.
The research evidence indicates that ERAS protocols is not likely to compromise on patient mortality, morbidity, and readmissions rates, however, outcomes of ERAS protocol varied across individual studies and reviews that make it challenging for researcher to determine the generalizability and feasibility of the research findings. Thus, the following chapter has included systematic literature review to analyse evidence that has reported ERAS programs’ effectiveness in improving quality of life and mortality rate amongst elderly patients with gastric or colorectal cancer.
A study conducted by Wang et al. (2012) evaluated that the length of post-operative stay and readmission rates are likely to be reduced in elderly patients receiving ERAS programmes comparatively to elder patients who received conventional treatment or care protocol.
The research evidence or findings of the study is based preliminary on gastric or colorectal surgery and the feasibility of results to other specialities of surgery remains uncertain. Thus, the following research question has been formulated based on PICO framework mentioned in the table below:
| To what extent is the ERAS programme useful for reducing length of post-operative stay and readmission rates in gastric/colorectal elderly patients? | |
|---|---|
| Population | Elderly post-operative colorectal/gastric patients |
| Interventions | ERAS (Enhancing Recovery After Surgery) |
| Comparator | Being on ERAS programme against not being on ERAS programme |
| Outcome | Reduced length of stay and readmission rates |
Table 1: Context of PICO Framework
Professional editors proofread and edit your paper by focusing on:
To conduct the following systematic review, several significant prospective and retrospective studies have been identified. The studies relevant to the chosen topic have been selected based on inclusion and exclusion criteria, databases, and literature search strategy.
The following systematic review of available and significant research evidence has been performed using databases such as CINAHL, Google Scholar, EBSCO, ProQuest, MEDLINE, Science Direct, etc. Apart from these databases, published protocol of ERAS programmes for gastric and colorectal cancers have also been used in this study to gather reliable and valid research findings for analysing the usefulness of ERAS programme in reducing readmission rates and length of post-operative stay in gastric/colorectal elderly patients.
The inclusion and exclusion criteria of the following study are mentioned in the tables below:
| Inclusion Criteria | Rationale |
|---|---|
|
|
|
|
|
|
|
|
|
|
Table 2: Inclusion Criteria of the Study
| Exclusion Criteria | Rationale |
|---|---|
|
|
|
|
|
|
|
|
Table 3: Exclusion Criteria of the study
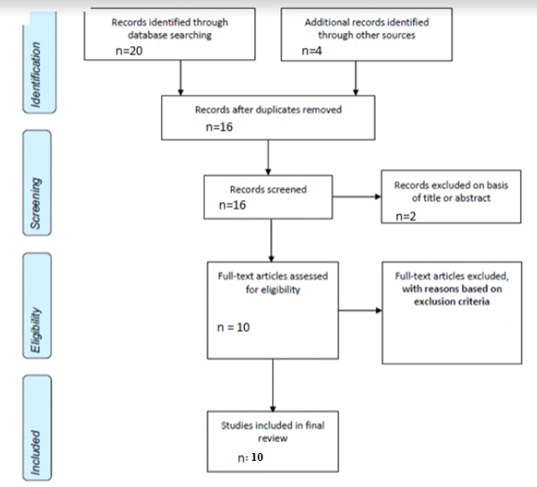
In the following research study, the literature searching was performed using PRISMA strategy and Boolean searching strategy. Boolean searching strategy included different key words that enabled researcher to gather information and research evidence based on important key words typed on various databases.
The key words used in the literature included ERAS programmes or protocol, effect of on length of stay and readmission rates, effect of on length of stay after surgery at hospitals, and reduced rate of readmissions in gastric or colorectal elderly patients. AND, OR, and NOT during the literature searching were also used as a Boolean Operators. On the other hand, PRISM strategy that has been used to select relevant studies and articles is outlined in the below mentioned flow chart:
A study conducted by Aarts et al. (2012) used a retrospective cohort study to examine the adoption of ERAS strategies for decreasing complications, fasten recovery, and reduced hospital stay in patients who underwent colorectal surgery. The study’s findings emphasised that the uptake of ERAS programmes and strategies is significantly associated with the shortened length of stay and readmission cases in patients undergoing colorectal surgery within the healthcare facility.
The study results have significantly contributed to total reduced length of stay at hospital that was 6.5 days with an average of 8.6 days. In addition to this, the bivariate analysis of the study revealed that ERAS strategies were associated with a hospital stay of less than 5 days and found that ERAS strategies effectively reduce post-operative length of stay and readmission cases in colorectal elderly patients.
The study also demonstrated that there are various types of ERAS strategies associated with reduced length of hospital stays, including preoperative counselling about expected length of stay, clear fluid on the day of surgery, intraoperative fluids restriction, and discontinuation of Foley catheter during 24 hours of colon surgery and 72 hours of rectal surgery.
One of the major strength of this study is that it has provided good evidence to other types of interventions that could significantly results into a shortened post-operative length of stay and accelerated recovery. However, the study has been found limited and suffers from the weaknesses relevant to the methodology used in the study.
Due to non-experimental design, the researcher was only able to find the association between adoption of ERAS strategies and length of stay and found causal relationship between each other and did not find variables that have association with shortened length of stay.
On the other the study of Pędziwiatr et al. (2015) found that the introduction of ERAS programme or protocol has compliance level of 80% and initial stage of preoperative and post-operative duration should be put on continuous evaluation and training of personnel with ERAS protocol for acquiring positive results in terms of reduced length of stay and post-operative complications.
The study also emphasised that the early implementation of ERAS protocol allows improvement of the post-operative results. However, it is relied on the appointment of an ERAS coordinator following constant analysis and auditing of the outcomes, along with the establishment of multidisciplinary ERAS team.
It has identified that ERAS protocol is an effective approach that significantly improves the overall perioperative and post-operative care. Ljungqvist (2014) supports these findings and stated that the most effective way to improve perioperative care is to establish ERAS protocol and develop a multidisciplinary team responsible for its effective implementation.
The article is noteworthy for providing additional and valuable information that the early implementation of ERAS protocol is essential for improving perioperative care that ultimately results in reduced length of stay and readmission cases particularly among elder patients with colorectal cancer. However, the major weakness that have been found in this study is the utilisation of own results and observations showed biasness in research findings that may affect the attitudes of staff and reduce the effectiveness of ERAS protocol.
In addition, the study conducted by Pędziwiatr et al. (2016) reported that laparoscopic rectal cancer surgeries are associated with increased length of stay at hospitals compared to colonic resections, despite implementing ERAS protocol during perioperative care.
The factors that have been found associated with the increased hospital stay include post-operative drainage, bowel preparation, and de-functioning ileostomy. It revealed that the there is a necessity for applying all the essential elements of the protocol during perioperative care that can be evaluated in future studies of this subject.
A major weakness of this study is that it did not observe the parameters of post-operative care as mobilization on the day of the protocol and evaluation of tolerance of oral diet on the first day of post-operative care that result in effectiveness of ERAS protocol in colorectal elderly patients.
On the contrary, the study of Christensen et al. (2011) found that the implementation of ERAS protocol as a fast track strategy in patients after open elective colonic surgery is significant for reducing the length of stay and considered as a safe protocol.
Moreover, it has also identified that the introduction of fast-track multimodel seemed to reduce the number of complications and length of stay at hospitals at open colon surgery. From this analysis, it could be concluded that all strategies or interventions should be made per the ERAS protocol to ensure success of fast track protocol with the reduction of length of post-operative stay at hospitals. However, the selection of laparoscopy opposed to open surgery has not seemed to be an important factor for the study and made findings quite irrelevant to the study theme.
In addition, Gonzalez-Ayora, et al. (2016) stated that ERAS pathway after colorectal surgery in elderly patients has proven to improve perioperative care and results in reduced hospital stay and morbidity rate after colorectal surgery. This protocol has been found feasible and safe for elderly patients based on valid and reliable reported outcomes of complications, compliance rates, needs for reoperation, and readmissions.
This study has considerable limitations such as the study has not compared results of elderly patients to a control group of patients who were <70 years old with the same protocol of ERAS, lack of significant data in previous studies, and not conduced as a randomized clinical trial to establish robust and valid conclusions.
In contrast, a research conducted by Wong-Chong, Kehlet, and Grantcharov (2016) evaluated that laparoscopic gastrectomy associated with ERAS protocol influence significantly on length of stay during perioperative care and results in shortened length of hospital stay with an acceptable mortality and morbidity rate.
This study has provided comprehensive perioperative outcomes by an ERAS programme, particularly for laparoscopic gastrectomy. The protocol suggested for ERAS programme included no use of gastrointestinal tubes, early oral intake, no use of epidural analgesia, or drains, planned discharge followed by completion of 72 hours after operation, and early removal of urinary catheters.
The study found average length of stay after implementing ERAS programme during perioperative care initially 7-19 days in conventional perioperative care. The limitation of this study is that it has not determined potential delayed complications, including criticisms and other long-term oncologic outcomes like overall survival rate and disease-free status. However, the study has presented laparoscopic gastrectomy as having an efficacy and safety similar to that of open gastrectomy with an ERAS protocol.
Furthermore, the study of Feroci et al. (2013) identified improved short-term outcomes in patients underwent colorectal surgery performed along with an ERAS programme when compared with standard care protocol. In addition, the effect of patient factors on post-operative outcomes have also been identified in this study and found that the outcomes of ERAS protocol is not influenced by factors such as BMI, sex, rectal or colonic surgery. However, age factor older than 75 years is considered an important influential independent factor that negatively impacts length of stay, mortality, and morbidity rate.
Furthermore, the study of Baird et al. (2010) reported that the elderly patients that have been gone through laparoscopic colorectal surgery on ERAS programme discharge results in increased recovery outcomes in terms discharge of patient one day sooner than elderly patients on conventional care or recovery programmes.
It asserts that ERAS as fast-track programmes is essential for reducing length of stay in colorectal surgery and could improve surgical complications and readmission cases in colorectal or gastric elderly patients. The study significantly proves that the advantages of ERAS programmes not only for the patients, but also for healthcare management, as cost of inpatient beds are substantially decreased and elder patients could be discharged more sooners than patient receiving traditional care protocol and return to their normal life more quickly.
However, due to the limited number of elder patients who participated in a formal preoperative training or educational program in this particular retrospective study, the researchers could not depict a correlation between post-operative outcomes and preoperative education that shows a major limitation of this study.
On the other hand, the study of Bona, et al. (2014) evaluated and confirms that the integration of an intervention of ERAS in colorectal surgery facilitate expeditious post-operative recovery and decreases the duration of post-operative stay comparatively to patients associated with traditional care protocol.
The findings of the study also revealed that the implementation of ERAS pathway in elder patients for colorectal surgery is highly effective, realistic, and feasible that allows care protocol with high compliance and thus considered as an immediate post-operative recovery pathway or programme results in shortened the length of stay and readmission rates.
It asserts that this prospective study is a noteworthy and remarkable evaluation of ERAS effectiveness as the study’s findings confirm that the implementation of ERAS protocol shortens the rate of hospitalisation and allows quicker post-operative recovery.
The study of Stephen and Berger (2003) also found that the implementation of ERAS protocol allows improvement of the post-operative results after elective colon resection. The integration of a clinical pathway for open, elective, colon resections could safely be performed done with improvements length of stay and cost of longer length of post-operative stay.
The findings of the prospective and retrospective studies included in this systematic review asserted that ERAS is a standardised framework that has been implemented extensively for attaining significant improvements in reducing post-operative length of stay at hospitals.
Aarts, M.A., Okrainec, A., Glicksman, A., Pearsall, E., Victor, J.C. and McLeod, R.S., 2012. Adoption of enhanced recovery after surgery (ERAS) strategies for colorectal surgery at academic teaching hospitals and impact on total length of hospital stay. Surgical endoscopy, 26(2), pp.442-450.
Baird, G., Maxson, P., Wrobleski, D. and Luna, B.S., 2010. Fast-track colorectal surgery program reduces hospital length of stay. Clinical Nurse Specialist, 24(4), pp.202-208.
Bona, S., Molteni, M., Rosati, R., Elmore, U., Bagnoli, P., Monzani, R., Caravaca, M. and Montorsi, M., 2014. Introducing an enhanced recovery after surgery program in colorectal surgery: a single center experience. World Journal of Gastroenterology: WJG, 20(46), p.17578.
Bona, S., Molteni, M., Rosati, R., Elmore, U., Bagnoli, P., Monzani, R., Caravaca, M. and Montorsi, M., 2014. Introducing an enhanced recovery after surgery program in colorectal surgery: a single center experience. World Journal of Gastroenterology: WJG, 20(46), p.17578.
Christensen, H.K., Thaysen, H.V., Rodt, S.Å., Carlsson, P. and Laurberg, S., 2011. Short hospital stay and low complication rate are possible with a fully implemented fast-track model after elective colonic surgery. European Surgical Research, 46(3), pp.156-161.
Fazel, S., Geddes, J.R. and Kushel, M., 2014. The health of homeless people in high-income countries: descriptive epidemiology, health consequences, and clinical and policy recommendations. The Lancet, 384(9953), pp.1529-1540.
Feroci, F., Lenzi, E., Baraghini, M., Garzi, A., Vannucchi, A., Cantafio, S. and Scatizzi, M., 2013. Fast-track surgery in real life: how patient factors influence outcomes and compliance with an enhanced recovery clinical pathway after colorectal surgery. Surgical Laparoscopy Endoscopy & Percutaneous Techniques, 23(3), pp.259-265.
Gonzalez-Ayora, S., Pastor, C., Guadalajara, H., Ramirez, J.M., Royo, P., Redondo, E., Arroyo, A., Moya, P. and Garcia-Olmo, D., 2016. Enhanced recovery care after colorectal surgery in elderly patients. Compliance and outcomes of a multicenter study from the Spanish working group on ERAS. International journal of colorectal disease, 31(9), pp.1625-1631.
Jia, Y., Jin, G., Guo, S., Gu, B., Jin, Z., Gao, X. and Li, Z., 2014. Fast-track surgery decreases the incidence of post-operative delirium and other complications in elderly patients with colorectal carcinoma. Langenbeck’s archives of surgery, 399(1), pp.77-84.
Ljungqvist, O., 2014. ERAS—Enhanced Recovery After Surgery. Journal of Parenteral and Enteral Nutrition, 38(5), pp.559-566.
Muller, S., Zalunardo, M.P., Hubner, M., Clavien, P.A. and Demartines, N., 2009. A fast-track program reduces complications and length of hospital stay after open colonic surgery. Gastroenterology, 136(3), pp.842-847.
Pędziwiatr, M., Kisialeuski, M., Wierdak, M., Stanek, M., Natkaniec, M., Matłok, M., Major, P., Małczak, P. and Budzyński, A., 2015. Early implementation of Enhanced Recovery After Surgery (ERAS®) protocol–compliance improves outcomes: a prospective cohort study. International Journal of Surgery, 21, pp.75-81.
Pędziwiatr, M., Pisarska, M., Kisielewski, M., Major, P., Mydlowska, A., Rubinkiewicz, M., Winiarski, M. and Budzyński, A., 2016. ERAS protocol in laparoscopic surgery for colonic versus rectal carcinoma: are there differences in short-term outcomes?. Medical Oncology, 33(6), p.56.
Pędziwiatr, M., Pisarska, M., Kisielewski, M., Major, P., Mydlowska, A., Rubinkiewicz, M., Winiarski, M. and Budzyński, A., 2016. ERAS protocol in laparoscopic surgery for colonic versus rectal carcinoma: are there differences in short-term outcomes?. Medical Oncology, 33(6), p.56.
Shida, D., Tagawa, K., Inada, K., Nasu, K., Seyama, Y., Maeshiro, T., Miyamoto, S., Inoue, S. and Umekita, N., 2015. Enhanced recovery after surgery (ERAS) protocols for colorectal cancer in Japan. BMC surgery, 15(1), p.90.
Stephen, A.E. and Berger, D.L., 2003. Shortened length of stay and hospital cost reduction with an accelerated clinical care pathway after elective colon resection. Surgery, 133(3), pp.277-282.
Sugisawa, N., Tokunaga, M., Makuuchi, R., Miki, Y., Tanizawa, Y., Bando, E., Kawamura, T. and Terashima, M., 2016. A phase II study of an enhanced recovery after surgery protocol in gastric cancer surgery. Gastric Cancer, 19(3), pp.961-967.
Wang, G., Jiang, Z.W., Xu, J., Gong, J.F., Bao, Y., Xie, L.F. and Li, J.S., 2011. Fast-track rehabilitation program vs conventional care after colorectal resection: a randomized clinical trial. World journal of gastroenterology: WJG, 17(5), p.671.
Wang, Q., Suo, J., Jiang, J., Wang, C., Zhao, Y.Q. and Cao, X., 2012. Effectiveness of fast‐track rehabilitation vs conventional care in laparoscopic colorectal resection for elderly patients: a randomized trial. Colorectal Disease, 14(8), pp.1009-1013.
Wong-Chong, N., Kehlet, H. and Grantcharov, T.P., 2016. Outcomes from an enhanced recovery program for laparoscopic gastric surgery. Surgical Laparoscopy Endoscopy & Percutaneous Techniques, 26(3), pp.e50-e55.
| Reference | Intervention | Participants | Setting/context | Outcomes | Results | Methods/quality | Other notes |
|---|---|---|---|---|---|---|---|
| Aarts, et al. (2012) | Fifty patient charts were retrieved from the medical records of each hospital using the Canadian Classification of Interventions (CCI) coding system.
The ERAS interventions examined were those that had been included in ERAS protocols and assessed in previous randomized, controlled trials and surgeons with patients enrolled in the study were asked directly about their practice patterns and whether they routinely included these strategies for their elective colorectal patients |
A retrospective cohort study of 336 consecutive
Patients of 62 years |
Seven teaching hospitals affiliated with the University of Toronto
Department of Surgery |
A primary outcome variable was total length of stay
for the first 30 days following initial elective procedure, including days stayed during any readmissions within the first 30 days A short hospital stay was considered a priori to be 5 days or less |
Laparoscopic
approach (odds ratio (OR), 1.24; 95% confidence interval (CI), 1.12–1.38), preoperative counseling (OR, 1.26; 95% CI, 1.15–1.38), intraoperative fluid restriction (OR, 1.26; 95% CI, 1.15–1.37), clear fluids on day of surgery (OR, 1.09; 95% CI, 1.00–1.2), and Foley urinal catheter discontinued within 24 h of colon surgery and 72 h of rectal surgery (OR, 1.13; 95% CI, 1.01–1.27) |
Multivariable regression model variables
with P\0.1 were included in the model with the exception of two ERAS variables Use of an ‘‘oral bowel preparation’’ was excluded, because the data were of poor quality and[25% of the data were undeterminable as this variable was inconsistently reported in the patient chart |
|
| Pędziwiatr, et al. (2015) | The entire analysed group of patients was divided into 3 subgroups (30 patients) depending on the time from ERAS protocol implementation and analysed the compliance with the protocol and its influence on length of hospital stay, post-operative complications and readmission rate in different subgroups | Group included 92 patients (43F/49M) with colorectal cancer submitted to laparoscopic resection
during the years 2013-2014 |
The study conducted in university tertiary referral medical center | Outcomes of the study include shortened length of stay, acceleration of ERAS adoption, and reduction in readmission rates | The average compliance with the protocol differed significantly between groups and was 65% in group 1, 83.9% in group 2 and 89.6% in group 3. The compliance with subsequent protocol elements was different. The length of stay and complication rate was statistically different in analysed subgroups. The whole group demonstrated an inverse correlation between compliance and length of stay. | Perioperative care in all of them based on ERAS protocol consisting of 16 items. Its principles and discharge criteria were based on the guidelines of the ERAS Society guidelines | |
| Pędziwiatr, et al. (2016) | The analysis included consecutive prospectively registered patients operated for a colorectal cancer between January 2012 and September 2015. | Patients were divided into two groups (colon vs. rectum). Group 1 (colon) consisted of 150 patients and Group 2 (rectum) of 82 patients | This prospective analysis conducted in hospital setting in the period from January 2012 to September 2015 | The measured outcomes were:
length of stay (LOS), complication rate, readmission rate, compliance with ERAS protocol elements and recovery parameters (tolerance of early oral diet, mobilization and time to first flatus). |
There was no statistical difference in complication
rate (27.3 vs. 36.6 %) and readmissions (7.3 vs. 6.1 %). Compliance with the protocol was 86.9 and 82.6 %, respectively. However, in Group 1, the following procedures were used less frequently: bowel preparation (24 vs. 78.3 %) and postoperative drainage (23.3 vs. 71.0 %). |
StatSoft STATISTICA version 10 was used for statistical
analysis. For the purposes of further analysis, the entire group of patients was divided into 2 subgroups, depending on the location of the tumor (colon vs. rectum). |
|
| Christensen, et al. (2011) | A fast-track programme was fully implemented, with a dedicated staff and a schedule for all perioperative procedures which included provision of information to patients, surgical guidelines, mobilisation and post-operative care. All previously existing procedures were modified according to
previously published guidelines |
131 fast-tracked patients were compared with 39 control patients. | The study conducted at the Surgical Department P, THG, Aarhus University Hospital | Outcome measures were reduced length of hospital stay. | The fast track significantly reduced the median hospital
stay from 7 to 3 days (p ! 0.0001). There was no difference in complication rates between the two groups, and no major complications were observed after early discharge from the hospital. The readmission rate was 15% in the fast-track group and 16% with the control patients. |
Patients were scheduled for outpatient appointments on post-operative day 9
to receive information on histology, check clinical status and have skin stitches removed; a telephone contact with a dedicated nurse was scheduled 4 weeks after surgery as a final checkup; clinical follow-up was performed after 3 months |
|
| Gonzalez-Ayora, et al. (2016) | This is a multicenter observational study of a cohort
of elderly patients undergoing colorectal surgery within an ERAS program. |
A total of 188 consecutive patients over
70 years who underwent elective colorectal surgery within an ERAS program at three institutions during a 2-year period were included. |
A retrospective analysis was performed from the GERM
Group (Spanish for Grupo Español de Rehabilitacion Multimodal) prospective database by selecting patients ≥70 years, undergoing colon and rectal surgery following ERAS protocols in the last 2 years (2013–2014). |
Outcome measures were Mortality, Reoperations, Anastomotic leakage, Bowel ischemia, Hemoperitoneum, Internal hernia, Urinary tract injury, and Hospital length of staya | Early intake and early mobilization were the most
successfully carried out interventions. There was a global compliance rate of 56 % of patients for whom compliance was achieved with all measured interventions. The median hospital length of stay was 6 days. |
Patient baseline characteristics at the time of surgery, age,
gender, American Society of Anesthesiologists (ASA) score, major comorbidities, preoperative anticoagulation therapy were obtained from each patient’s electronic medical record. |
|
| Wong-Chong, Kehlet, and Grantcharov (2016) | This was a prospective study of consecutive patients undergoing elective laparoscopic gastrectomy combined with an enhanced recovery (fast-track) program. | 86 patients, 60 underwent partial gastrectomy and 26 underwent total gastrectomy | All procedures were performed by the same surgeon, at a single academic center, between 2008 and 2012. | Outcomes included the length of hospital stay, intraoperative and post-operative complications, the readmission rate, the reoperation rate, and the 30-day mortality. | The median length of hospital stay was 4 (range, 1 to 44) days. The conversion rate to open surgery was 11.6%. Four patients (4.7%) had an anastomotic leak. Three patients had post-operative bleeding (4.7%). About 4.7% (n = 4) of the patients required readmission and 8.1% required reoperation (n= 7). The 30-day mortality rate was 2.3% (n= 2) due to complications from anastomotic leak. | Billroth II gastrojejunostomy was performed for the first several cases using a linear stapler. All subsequent patients undergoing distal and subtotal gastrectomies underwent Roux-en-Y reconstruction. The procedure was modified from a Billroth II to a Roux-en-Y reconstruction due to the significant risk of bile reflux and gastritis with the former procedure | |
| Feroci, et al. (2013) | Three fellowship-trained colorectal surgeons carried out or supervised both the open and laparoscopic procedures and were involved in all of the surgeries.
The nasogastric tube, inserted after the orotracheal intubation, was always removed at the end of surgery in an ERAS intervention |
A total of 606 patients with colorectal pathology from 2005 to 2011 were analyzed to assess the relationships between patient factors, the outcome variables, and the items of the FT program | After institutional Review Board approval, we performed a query of a prospectively maintained divisional database (retrospective analysis) to identify all the patients (ASA grades 1 to 4) who underwent elective colorectal resection between January 1, 2005, and November 30, 2011, at our institution (a general surgery unit at a high-volume nonacademic tertiary-care hospital, not specializing in colorectal surgery). | Post-operative outcomes include mortality, morbidity, readmission rate, and length of post-operative hospital stay. | The median length of stay was 5 days, and readmission rate was 2.3%. The morbidity rate was 26.7%. Independent predictors of prolonged length of stay were older than 75 years of age, ASA grade 3 and 4, and the presence of an ileostomy. Independent predictors of morbidity were age above 75 years old and ASA grade, whereas age was confirmed as an independent predictor of mortality. | A univariate analysis was performed using the Mann-Whitney U test for continuous variables, and a w2 test was used for categorical variables. | |
| Baird, et al. (2010) | This study compared outcomes of a fast-track post-operative intervention implemented for patients undergoing laparoscopic colorectal surgery on 2 surgical units to patients receiving traditional post-operative care following laparoscopic colorectal surgery prior to implementation of the fast-track program | Two groups of patients assigned with traditional or ERAS protocol | The study was conducted at a large Midwestern hospital | Outcomes of the study is the correlation between preoperative education and post-operative outcomes | A statistical significant difference of 1 day was found between patients receiving traditional care and patients on the fast-track program. Readmission rates between the 2 groups were not statistically significantly different. | A retrospective medical record review was done on 100 patients who underwent laparoscopic colorectal surgery on the fast-track program for data pertaining to the research questions. | |
| Bona, et al. (2014) | A prospective evaluation of
compliance to a protocol based on full application of all ERAS principles, through the progressive steps of its implementation, were performed. Results achieved in the initial pilot study conducted by a dedicated team (n = 47) were compared to those achieved in the shared protocol phase (n = 143) three years later. |
143 patients underwent colorectal resection with ERAS perioperative management protocol. Median age was 64 years | This study was conducted by a restricted
multidisciplinary team within the clinical setting of the Day Surgery Unit |
Outcomes were length of post-operative hospital stay, readmission rate, compliance to the protocol and morbidity. | During the initial pilot study (March 2009 to December 2010; 47 patients) conducted by a dedicated multidisciplinary team, compliance to the items of ERAS protocol was 93%, with a median length of hospital stay (LOS) of 3 d. Early anastomotic fistulas were observed in 2 cases (4.2%), which required reoperation (Clavien-Dindo grade Ⅲb). | The ongoing organization of training events involving
health professionals involved only partially contributed to resize cultural barriers, through the sharing of the theoretical basis of the ERAS protocol and the practical aspects of its implementation. |
|
| Stephen and Berger (2003) | One hundred thirty-eight patients underwent elective colon resections at our institution by a single surgeon before (n = 52) and after (n = 86) introduction of a clinical pathway. Length of stay, post-operative complications, readmissions, and cost per patient were compared between the 2 groups | The study period began in August 1997, when
the senior author started his clinical practice at the hospital, and included all of his patients who underwent elective colon resections for cancer or diverticular disease from August 1997 through December 2000. |
The clinical pathway was instituted within the hospital setting. The pathway was designed with
the aim of providing optimal care in a cost-effective manner and consisted of the following |
The average hospital stay after colonic resection is 5 to 10 days. This study describes a clinical pathway for colon resections and examines patient outcome before and after institution of the pathway. | Mean total length of stay (± standard deviation [SD]) was less in the post-clinical pathway patients (3.7 ± 1.5 days) compared to preclinical pathway patients (6.6 ± 3.3 days) ( P < .001).
When adjusted for age, sex, diagnosis, and type of operation, the difference in length of stay remains statistically significant (P < .001). |
Clinical pathways were initially developed to
streamline the nursing care of post-operative patients8 and in recent years have come to include the participation of physicians and other non-physician health care workers, in addition to nurses. |
The purpose of the ERAS Program is to enhance patient outcomes by optimizing the entire surgical care process, focusing on preoperative preparation, intraoperative techniques, and postoperative recovery strategies.
You May Also Like
All work is written by human writers. 100% AI free, guaranteed.
100% money back guarantee if you find plagiarism in our work.
COMPANY DETAILS